TABLE OF CONTENTS
auteur
Senne Bonnaerens
Share



Rehabilitation works. Pain decreases, strength improves, and movement quality returns. Runners complete structured programs, meet return-to-run criteria, and regain confidence. Yet a consistent pattern remains: runners rarely get injured during rehab itself, but often after discharge. So the real question is not whether rehab works, but what happens after rehab.
The core of injury prevention is finding the right balance between the experienced cumulative load and the runner's load capacity. Running injuries mainly come down to two factors:
- Load tolerance: what the body can handle
- Load management: how load is applied over time
Injury occurs when cumulative load exceeds tissue capacity. Rehabilitation already addresses this well. Clinicians successfully rebuild strength, movement quality, and tissue capacity, creating the foundation for a safe return to run. But one key element becomes critical after rehab: how load is increased in real life.
Load tolerance adapts slowly
Musculoskeletal adaptation is slow by nature. Structural improvements can take months to a year, and even after extended training, long-term gains remain modest. Rehabilitation is much shorter by design. So at discharge, the runner is functionally ready, but biologically still adapting. At the same time, many runners reduce or stop strength work once symptoms disappear, slowing further adaptation.
The hidden gap: rehab vs running load
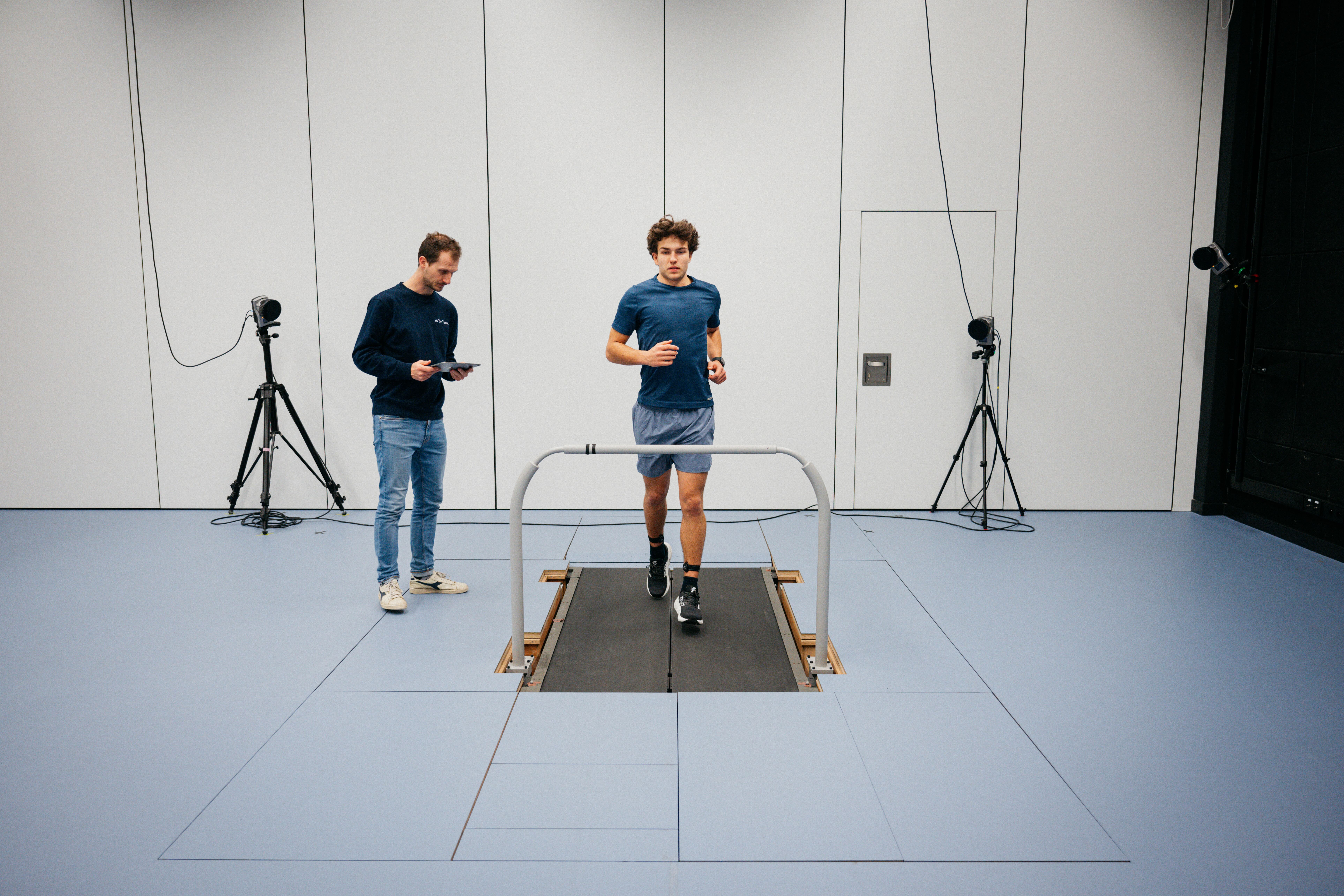
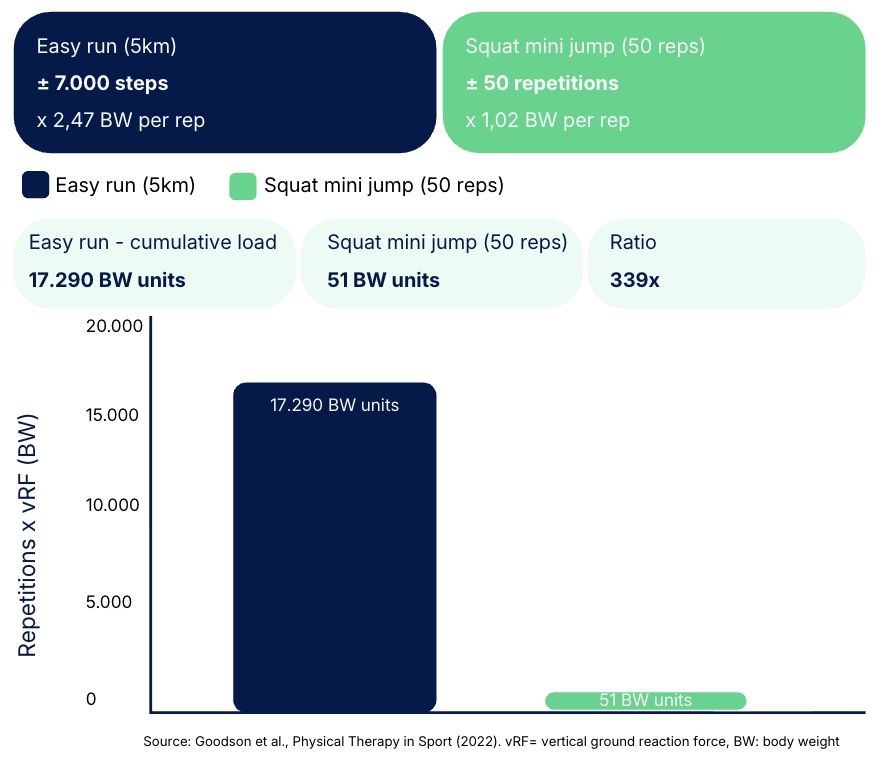
Research by Goodson et al. shows that one rehab repetition can equal the load of one running step. The difference lies in volume:
- Rehab: around 200 to 300 repetitions per session
- Running: thousands of steps per session
Even if tissues tolerate individual loads, they are not yet adapted to the repetitive nature of running.
Why injuries don't happen during rehab
During rehabilitation, external load is carefully managed and kept within safe limits. Progression is introduced gradually, patients are closely supervised, and adjustments are made when needed. This creates a stable balance between the load placed on the body and its ability to tolerate it, which is why rehabilitation is usually successful in reducing symptoms and restoring function.
Why injuries happen after rehab
The problems often start after discharge. Three things happen at the same time:
- Running volume increases quickly
- Supervision decreases
- Strength training is reduced or stopped
Meanwhile, load tolerance is still developing. This creates a mismatch: load increases faster than the tissue can adapt. That mismatch can appear within weeks and helps explain why rehab outcomes look successful, yet 50 to 70 percent of runners experience reinjury within one year.

Extending rehabilitation beyond the clinic
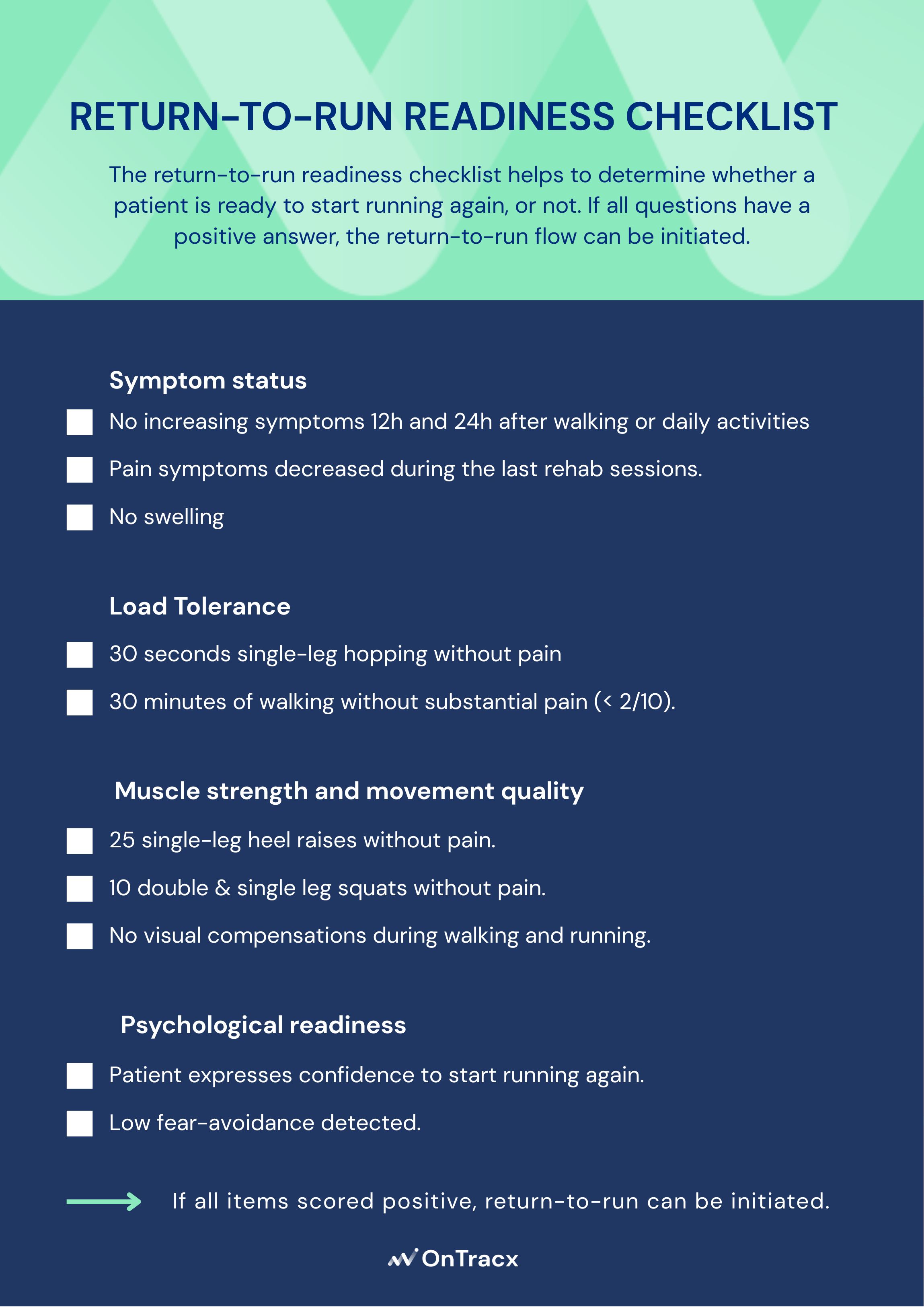
The key is to carry the principles of rehabilitation into the return-to-run phase, where most issues tend to emerge. This requires a clear starting load for each runner based on their injury history and current capacity, a gradual and individual progression of load, and insight into real-world running exposure outside the clinic. Rehabilitation is therefore not only about rebuilding capacity. It is also about guiding how load evolves once the runner returns to running.
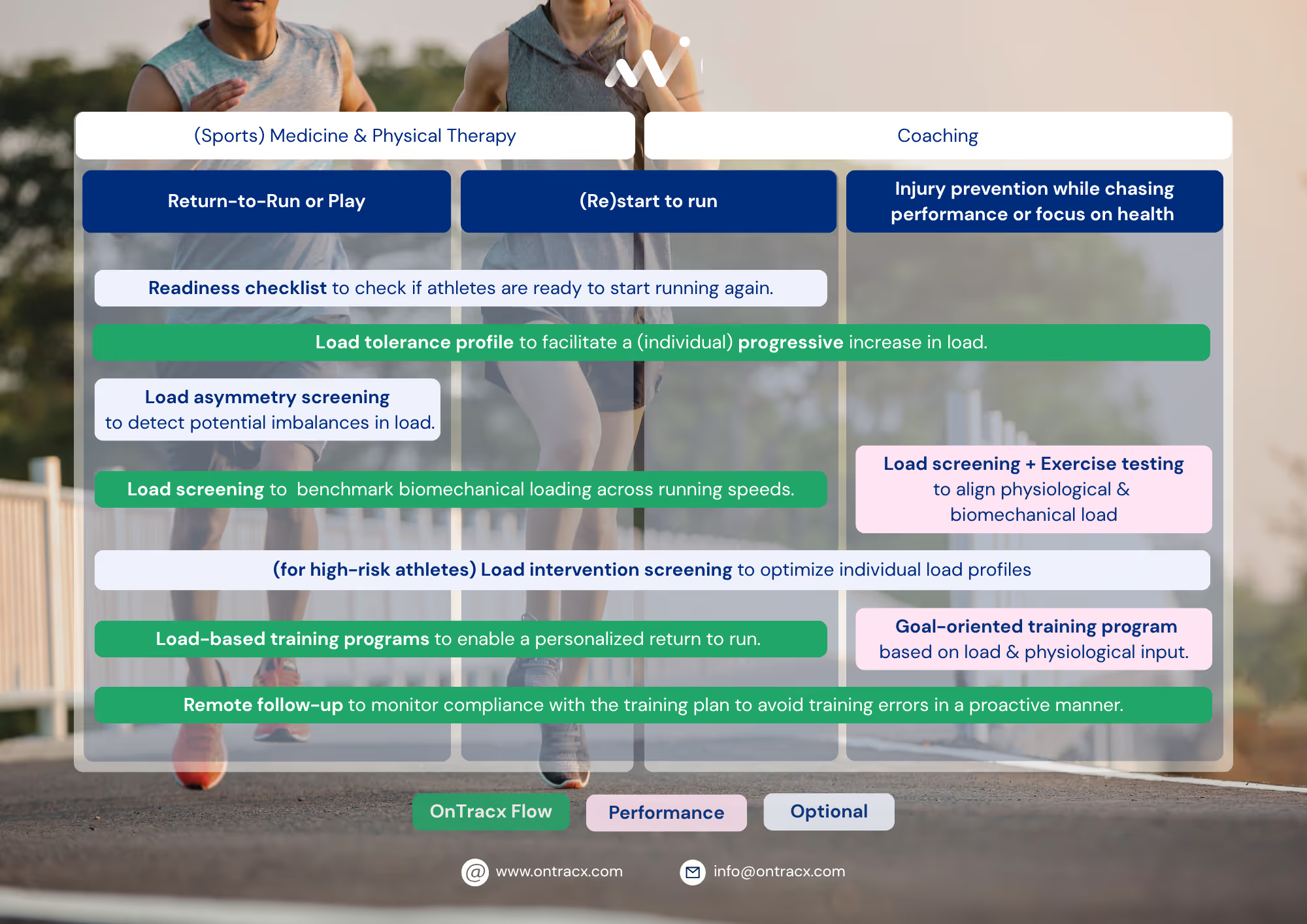
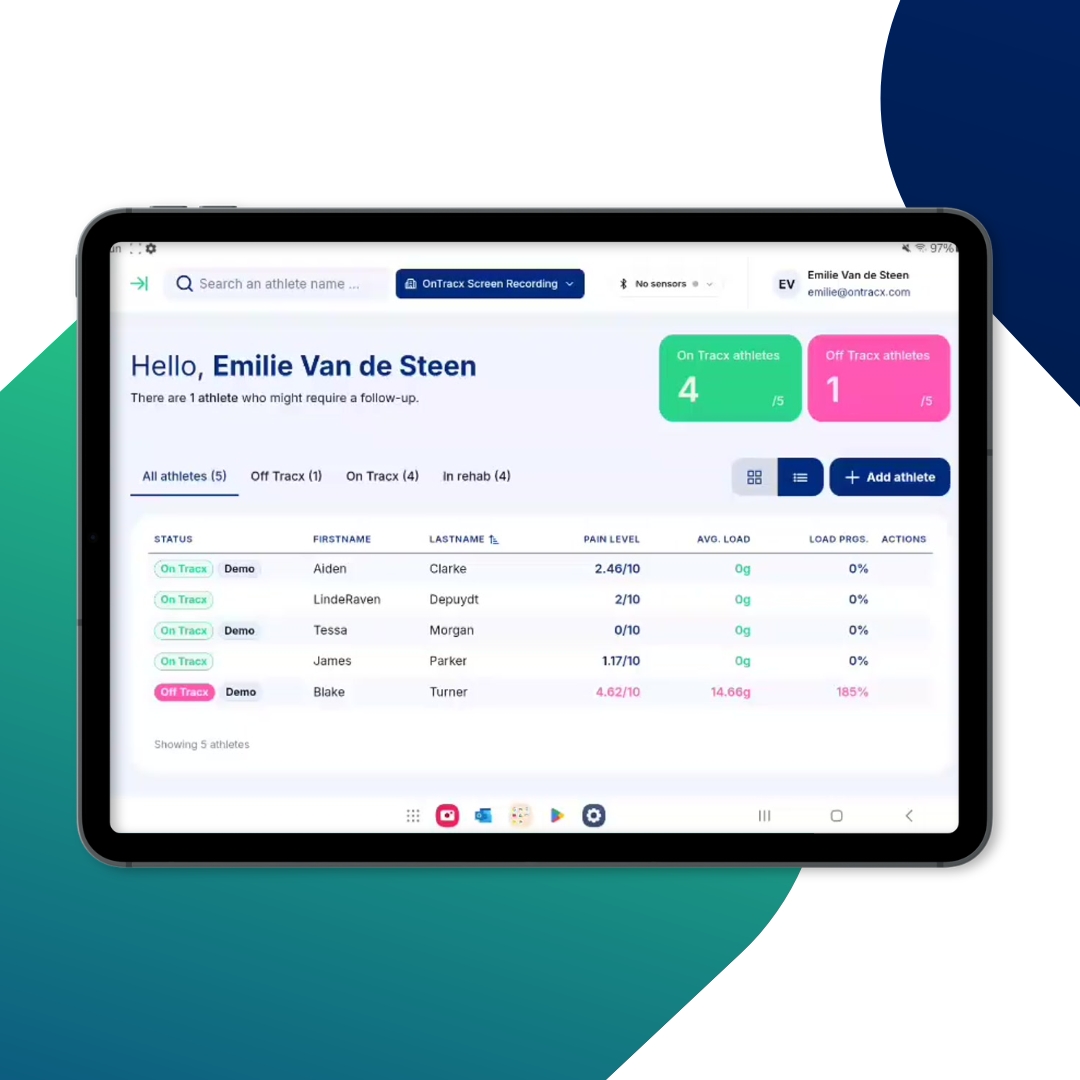
OnTracx extends rehabilitation beyond the clinic by bringing structured load management into real-world running, where most reinjuries actually occur. Instead of relying only on clinic-based progress, OnTracx makes the transition to return to run measurable, guided, and continuously adjustable.
This is done through three key components:
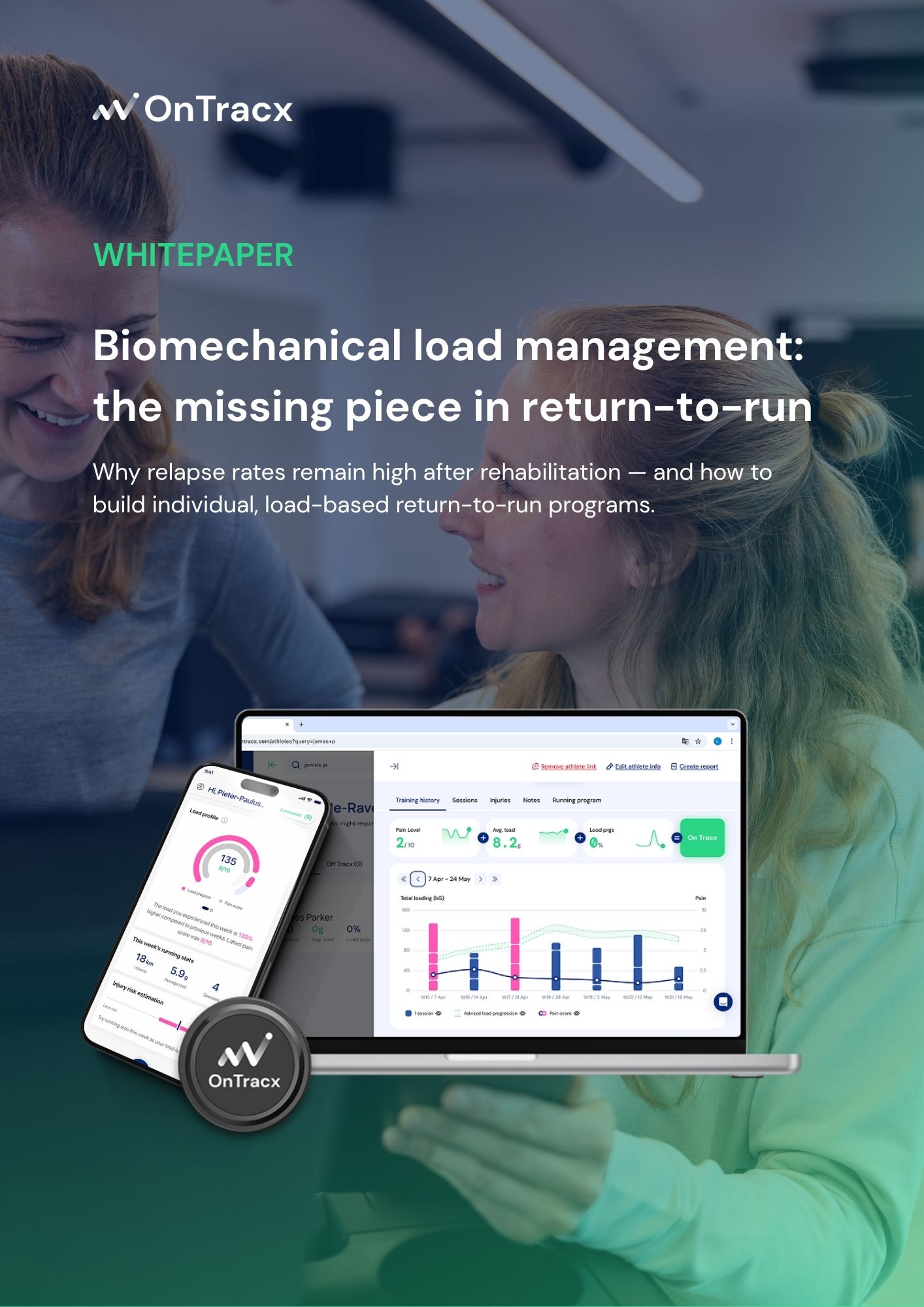
- Load screening: Wearable sensors measure biomechanical load during running on a step-by-step basis, providing objective insight into the actual stress a runner is exposed to.
- Load-based return-to-run programs: Personalised plans are built by combining injury history, running data, and individual load tolerance, allowing cumulative load to be progressed in a controlled and gradual way.
- Remote follow-up: Clinicians can continue monitoring runners after discharge by tracking load progression, training adherence, and symptom response, enabling timely intervention even outside the clinic.
Rethinking success in rehabilitation
If success is defined as a pain-free discharge and return to run, then rehabilitation is effective. But if success means a sustainable return without reinjury, one gap remains: load tolerance builds slowly, running load increases quickly, and the transition is rarely tightly controlled.
Conclusion
Rehabilitation does not fail runners, the transition does. Load is carefully controlled during rehab, but once discharged, that structure disappears at the very moment the body still needs it most. That is the gap worth closing.












%20(5).png)


%20(3).avif)
%20(4).avif)



.jpg)