TABLE OF CONTENTS
Share
Two ways to fight overuse injuries: build capacity and manage load
Most runners think injury prevention is mainly about becoming stronger. Stronger muscles, stronger tendons, better efficiency, and so on. And while all of that matters, it only tells half the story.
Running injuries rarely happen because the body is simply “weak.” They happen when the load applied to the body exceeds what the tissues can currently tolerate (Edwards, B. 2018). In other words, injury risk is determined by the constantly shifting balance between capacity and load.
That balance can be influenced in two ways: by improving the body’s ability to tolerate load, or by managing how load is applied over time. The problem is that runners, coaches, and even rehabilitation programs often focus heavily on one side while underestimating the other.
Building capacity: making the body more resilient
Improving tissue capacity forms the foundation of most rehabilitation and injury prevention programs. Through strength training, plyometrics, and progressive impact exposure, muscles become stronger, tendons adapt, and bones remodel in response to loading. Research consistently shows that sufficiently high mechanical stimulus is necessary to trigger meaningful adaptation, particularly in tendon and bone tissue (Mellon & Tanner, 2012; Gregov et al., 2014).
At the same time, the scientific literature around injury prevention in endurance runners is more nuanced than many assume. A recent systematic review and meta-analysis by Wu et al. (2024) found no clear overall reduction in running-related injury risk from exercise-based prevention programs compared to running alone. In this, many of the programs that failed to show benefit relied on relatively low-intensity or non-specific exercises, while higher-load strength and neuromuscular training have shown more promising results in other sports populations.
This suggests that the question is probably not whether exercise works, but rather which type of exercise, at what intensity, and for which tissue. Running injuries are highly repetitive and tissue-specific, meaning that generic low-load exercise routines may simply not provide enough stimulus to meaningfully improve resilience against running load.
There is also another important limitation that is often overlooked: tissues adapt slowly (Bohm et al., 2015; Kjaer et al., 2009; Magnusson et al., 2003). Cardiovascular fitness can improve within weeks, while tendons, bone, and connective tissue remodel over months. Even after symptoms disappear, tissue adaptation is still ongoing long after rehabilitation ends.
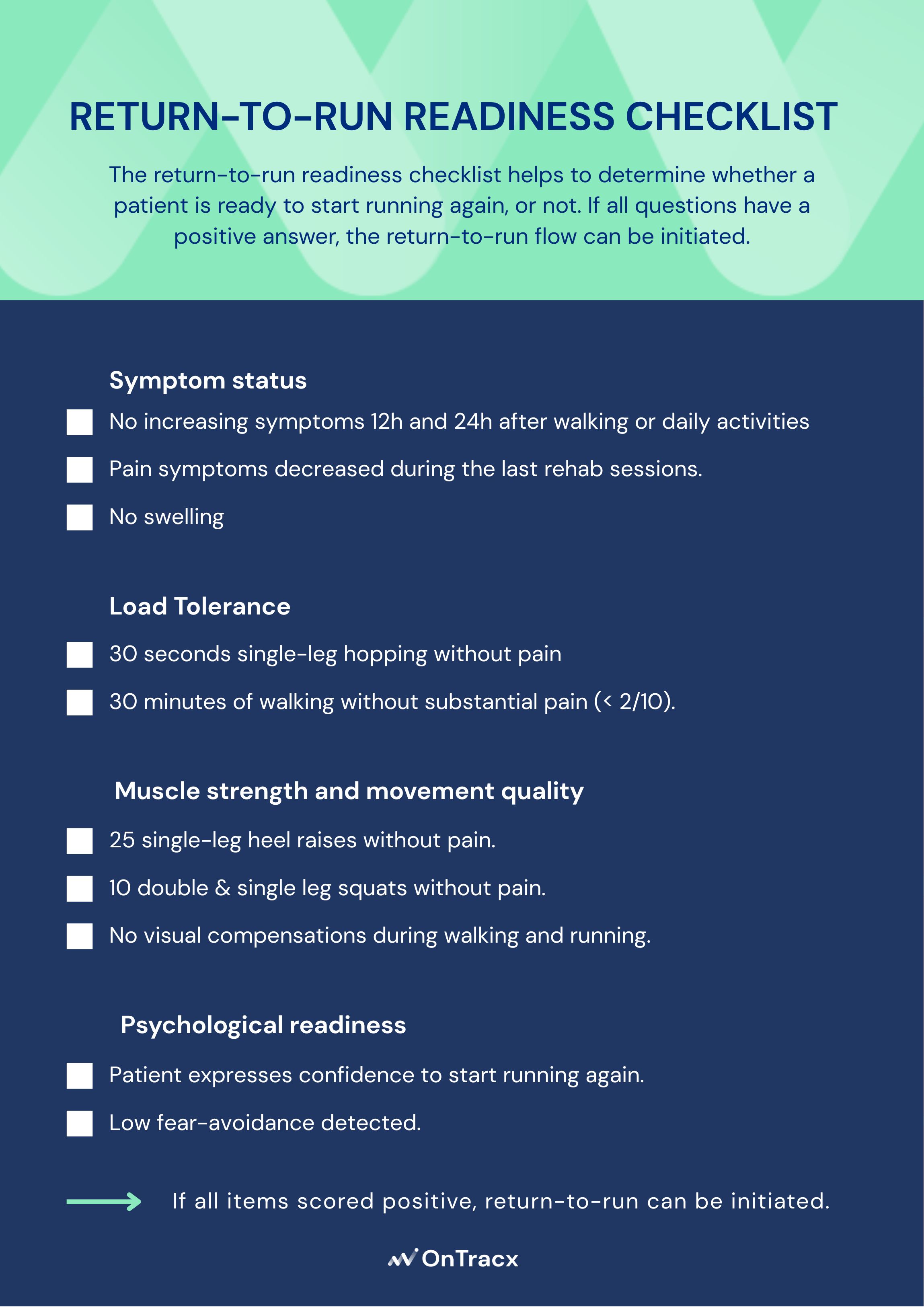
This creates one of the biggest challenges in running rehabilitation and injury prevention: runners often feel ready before their tissues truly are. Aerobic fitness, confidence, and performance tend to return much faster than mechanical tissue tolerance.
Why strength alone often fails
This is also why runners rarely get injured during rehabilitation itself, yet frequently relapse afterward.
During rehab, load is carefully controlled. Progression is gradual, exercises are supervised, and exposure remains relatively predictable. But once runners return to unrestricted training, running volume increases, supervision disappears, and strength work is often reduced at the exact moment tissues are still adapting.
The issue is not that rehabilitation fails, but that progression during and afterward is often poorly managed.
Running creates enormous cumulative mechanical load. Goodson et al. (2022) showed that individual rehab exercises can generate loads similar to running steps, but the difference lies in repetition volume. A rehab session may contain a few hundred repetitions, while even a short run generates thousands of impact cycles per leg.
That means a runner can leave rehabilitation feeling stronger and pain-free, while still not being fully prepared for the repetitive demands of real-world running.
Of course, the path from capacity to resilience also depends on the tissue and pathology involved. A tendinopathy and osteoarthritis, for example, respond to different loading stimuli and adapt on different timelines, which means rehabilitation strategies need to be fine-tuned rather than applied generically.
Managing load: the other half of injury prevention
If capacity determines what the body can tolerate, load management determines how quickly the body is asked to tolerate it.
This is where most overuse injuries develop: cumulative load quietly outpaces what tissues can adapt to, rarely as the result of one catastrophic session.
Mechanical load is also influenced by far more than just mileage. Speed, terrain, footwear, fatigue, and biomechanics all influence how much stress tissues experience with every step. Two runs of identical distance can therefore create completely different mechanical demands.
This is one of the reasons why generalized progression rules such as the “10% rule” often fail in practice. They only account for volume, while actual tissue stress may rise much more aggressively depending on how running load changes. In fact, per-step and cumulative load at common running injury sites can vary substantially with speed, surface gradient, and cadence alone (Van Hooren et al., 2024).
Successful injury prevention therefore depends not only on improving tissue capacity, but also on managing how quickly cumulative load evolves over time.
The goal is not less load — it is better load management
Managing load does not mean avoiding hard training or training conservatively forever. Mechanical loading is essential for adaptation. Without sufficient stress, tissues never become stronger.
The goal is not to avoid load, but to expose the body to load progressively enough for adaptation to occur without repeatedly exceeding tissue tolerance. That balance is highly individual and constantly influenced by recovery, training history, previous injuries, and running mechanics.
Nutritional status also shapes how well tissue tolerates load. A 2025 systematic review and meta-analysis found that low energy availability is associated with impaired bone health and a higher risk of bone stress injuries in athletes (Gallant et al., 2025). For runners, this means that even a well-designed loading program can underperform if energy intake does not match training demand.
This is why individualized progression matters so much. Not every runner responds to load in the same way, and not every injury is solved by simply adding more exercises.
Where technology changes the equation
The difficulty is that mechanical load is largely invisible. Runners can feel out of breath, but they cannot directly feel how much cumulative stress their tendons or bones are absorbing step after step. Symptoms often appear only after overload has already accumulated for days or weeks. Research suggests that runners may not always be aware of elevated mechanical strain: in one study, runners who later sustained an injury showed significantly higher cumulative biomechanical load than non-injured runners, despite reporting no difference in pain or fatigue (Kiernan et al., 2018). A more recent field study found that subjective effort ratings correlated only weakly with measured biomechanical load during outdoor running, reinforcing that perceived exertion is a poor proxy for actual mechanical stress (Scheltinga et al., 2026).
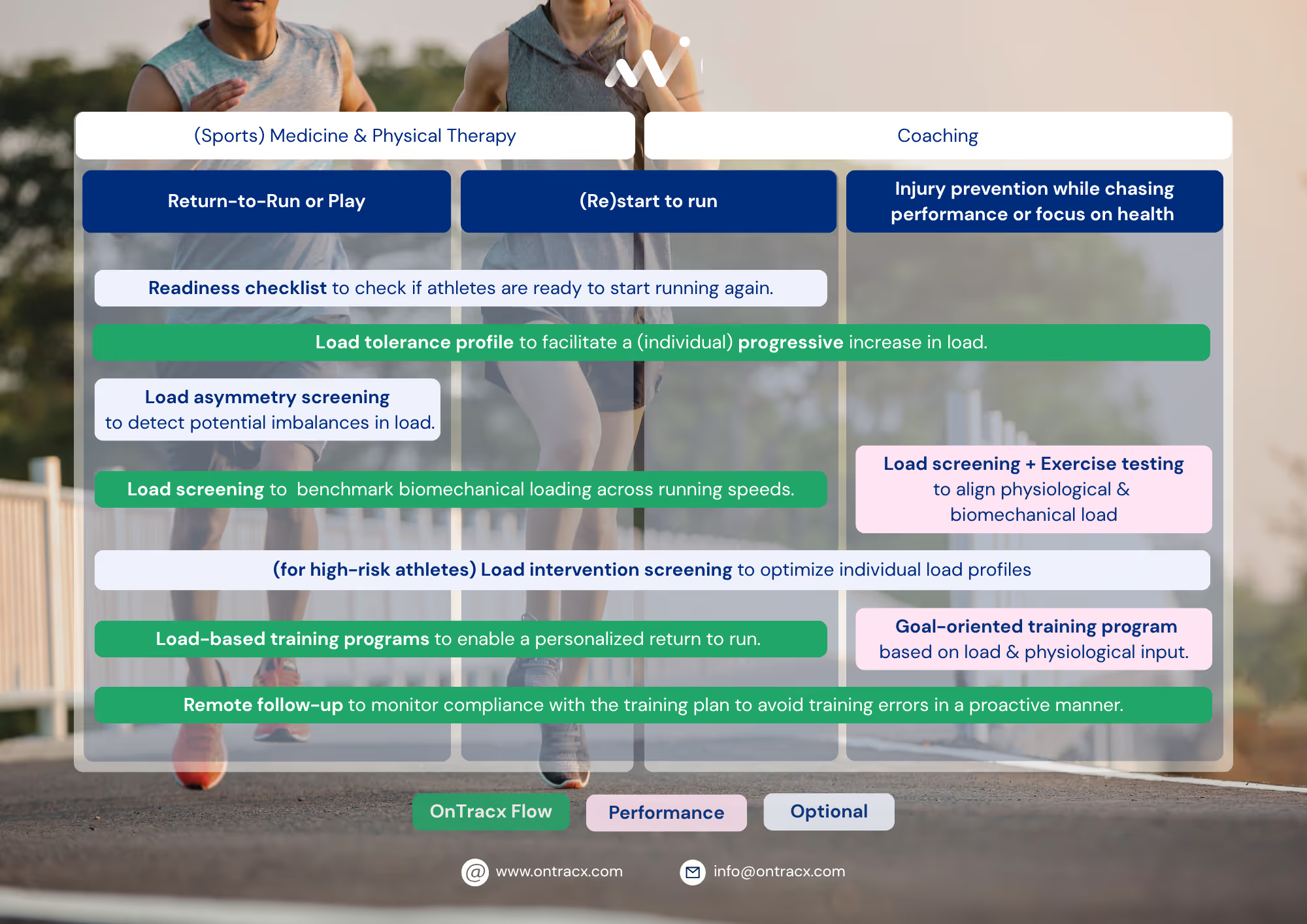
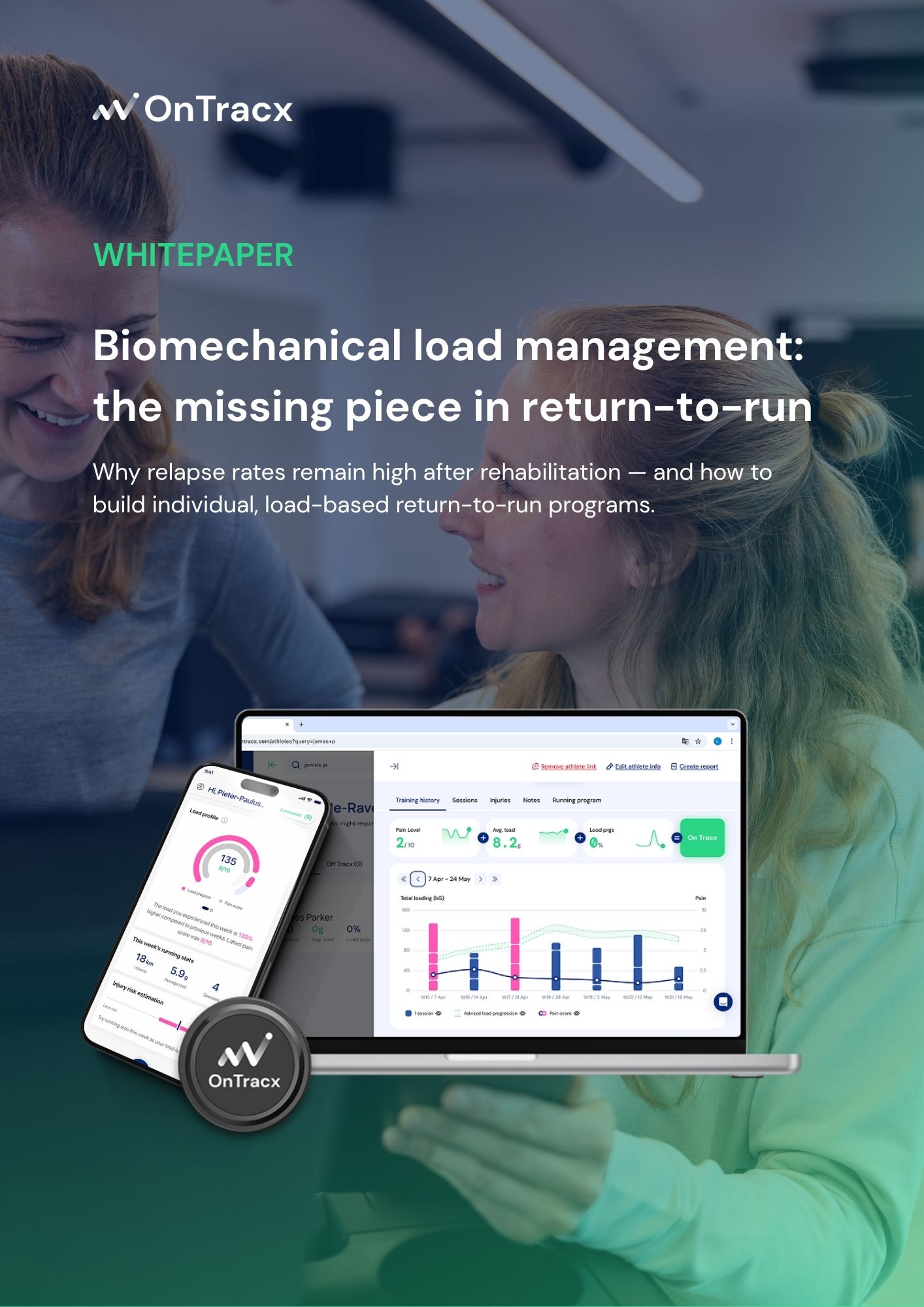
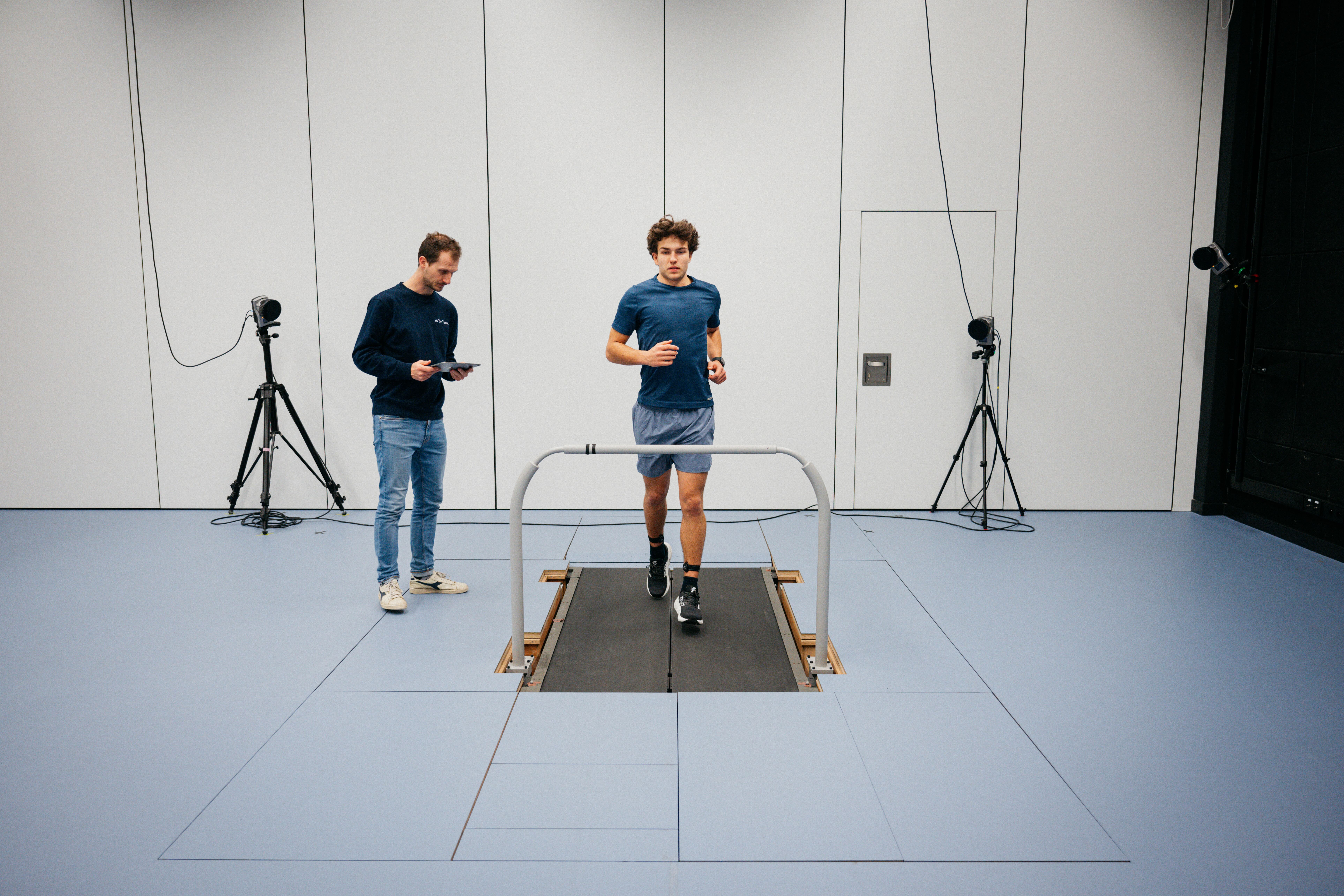
That is where objective load monitoring becomes valuable. By measuring mechanical load during running, OnTracx helps quantify how much impact load tissues are actually exposed to and how that load evolves over time. Combined with load screening and individualized load-based training plans, this allows progression to be adjusted not only based on performance goals, but also on load progression relative to individual tolerance.
This shifts progression away from guesswork and toward measurable load management. Not to make training more conservative, but to make progression more sustainable.
Too much to read
There are, broadly, two levers to reduce overuse injuries: improving the body's capacity to tolerate load, and improving how load is managed over time. Neither operates in isolation: recovery, mental health, pain coping, and nutrition all shape how well a runner adapts. Within a holistic approach, capacity building may currently receive disproportionate attention, not because it matters less, but because gradual load progression has historically been difficult to track and manage, and because many therapists have limited experience with what is, in essence, coaching and programming.
The most successful runners do both. They build stronger tissues through progressive strength and impact training, while simultaneously respecting the fact that adaptation takes time. Because overuse injuries are rarely caused by a single bad session. They develop when cumulative load quietly outpaces adaptation for long enough.
And preventing that requires more than simply getting stronger. It requires managing load just as intelligently as we train performance.










%20(5).png)


%20(3).avif)
%20(4).avif)





.jpg)