TABLE OF CONTENTS
Share
Patient profile
Age/sex: 31-year-old male
Goal: Pain-free running and build toward 10 km + trail running
Activity level: Runs 2–3×/week + gravel cycling + desk job
History: First symptoms after half marathon (Nov), ongoing for 6 months
Clinical presentation
Diagnosis and contributing factors
The patient presented with recurrent lateral knee pain consistent with Iliotibial Band Syndrome (ITBS), which developed after completing his first half marathon in November without a structured training progression. Since onset, symptoms repeatedly reappeared following independent return-to-run attempts, each time without a graded loading build-up.
Pain was localized to the lateral knee, presenting within 1–2 km of running and reaching up to 7/10 in intensity, forcing cessation of activity. Symptoms typically persisted for 1–2 days post-run and were also provoked by stair descent and prolonged walking.
Initial assessment revealed clear tenderness along the iliotibial band with increased tone in the TFL and gluteal complex. No imaging was performed.
Contextual load: The patient runs 2–3×/week, cycles to work on gravel 1–2×/week, and has a desk-based job. Strength training exposure was inconsistent. Running mechanics showed a low cadence (~150 spm) with a clear cross-over gait pattern. Previous return-to-run attempts consistently involved immediate 4–5 km continuous runs, exceeding current tissue capacity.
Treatment approach
In-clinic interventions
Initial treatment focused on reducing lateral chain irritability through manual therapy targeting the ITB, TFL, and gluteal musculature, combined with mobility work to reduce local tone and sensitivity.
Rehabilitation then shifted toward improving load tolerance through structured strength and stability training, with emphasis on hip control and single-leg loading capacity.
Gait retraining was introduced with two main objectives:
- increasing cadence (without increasing running pace)
- reducing cross-over gait to decrease lateral knee compression
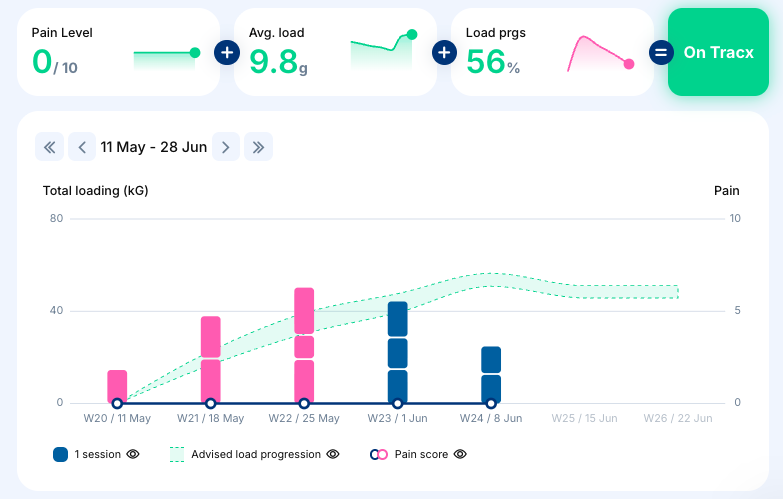
Return-to-Run program
Progression (start date: 11 May)
Phase 1 — walk/run intervals, 3×/week
Running was reintroduced using a conservative walk-run structure. Cadence and pace were controlled, with very gradual exposure to prevent symptom reactivation. Progression was continuously adjusted based on symptom response.
Phase 2 — gradual continuous running
Transition toward continuous running was introduced in small increments, prioritizing tissue adaptation over performance. Progression remained deliberately slow given the history of repeated flare-ups following rapid load increases.
Current status: approximately 3 weeks into the program, with running tolerance improving and symptoms remaining well controlled.
Target — 10 km + trail running capacity
Progression toward consistent 10 km running with a longer-term goal of trail running exposure.
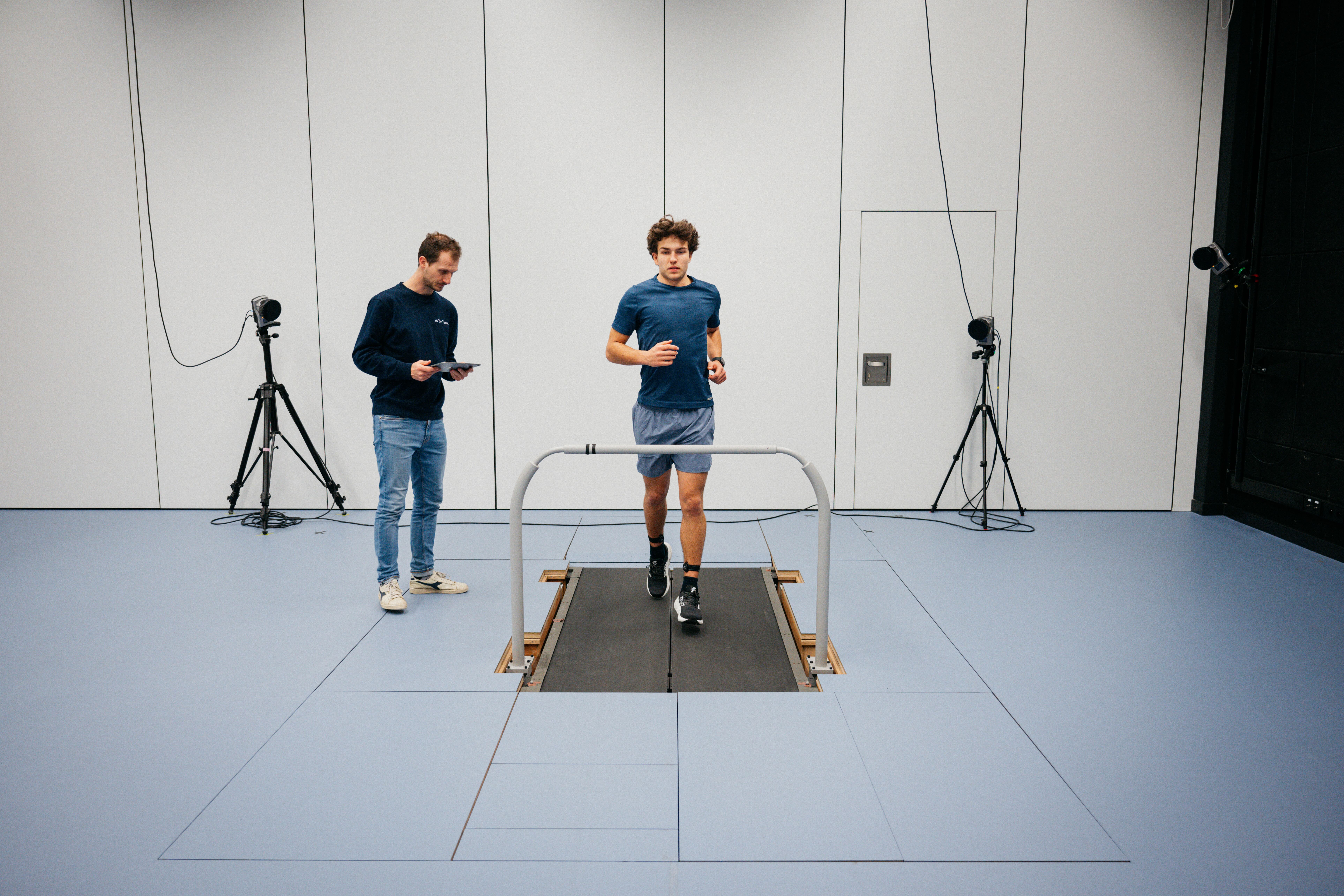
OnTracx findings
Value of field monitoring
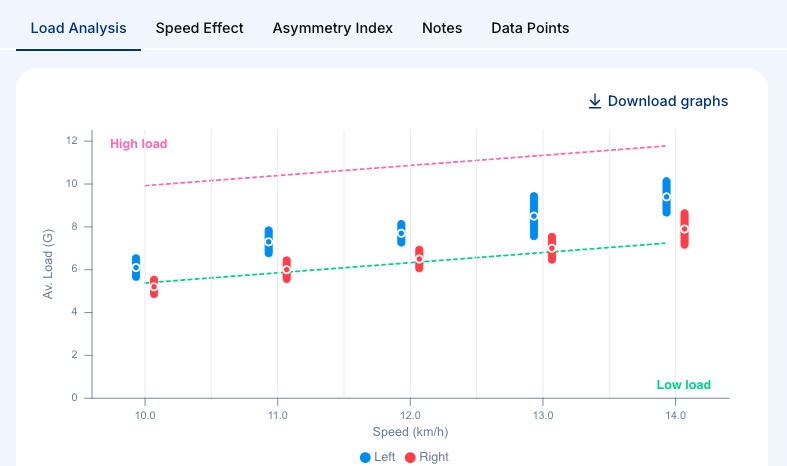
Screening revealed consistently low cadence (~150 spm) with a clear asymmetrical loading pattern and increased demand on the symptomatic lateral chain.
Despite this, the patient demonstrated the ability to run at higher speeds (up to ~14 km/h) without pain reproduction during testing, indicating that cardiovascular capacity exceeded current tissue tolerance.
Load distribution patterns suggested that symptoms were primarily driven by movement strategy and cumulative mechanical stress rather than absolute running intensity.
Clinical reasoning
Why this approach worked
The main issue was repeated premature exposure to excessive running load. Each prior attempt restarted with 4–5 km continuous runs, which exceeded current tissue capacity and triggered symptom recurrence.
A structured and gradual return-to-run approach allowed progressive tissue adaptation without overload. Strength work improved global load tolerance, while gait retraining reduced lateral knee compression during stance.
Cadence increase was a key intervention, likely reducing peak lateral knee load per step and improving overall movement efficiency. Combined with reduced cross-over gait, this decreased irritability of the iliotibial band during running.
Key clinical takeaway
💡This case shows that overuse symptoms are driven by early excessive mechanical load exposure relative to tissue tolerance, rather than overall running fitness or running endurance.
A gradual return-to-run plan with cadence and strength work helped control symptoms and rebuild sustainable running tolerance.












%20(5).png)


%20(3).avif)
%20(4).avif)





.jpg)